Abstract
Purpose. To determine whether hip range of movement (ROM) can predict the occurrence of adductor strain among male professional soccer players.
Methods. 120 subjects were prospectively selected from 6 professional soccer clubs in Australia. Internal rotation, external rotation, and ROM of the hip were measured using a goniometer before and during the course of a soccer season (2003–2004). When adductor strain occurred, further assessments of the hip were performed. Injured subjects’ hip ROMs were measured again at the end of the season.
Results. Eight of the 120 subjects had 9 adductor strains (one bilateral). There was a correlation between preseason decreased hip ROM and occurrence of adductor strain. The mean preseason hip ROM was 44.7 degrees in the injured group and 53.7 degrees in the uninjured group. Once the subjects were able to resume playing soccer, their hip ROM increased to near pre-injury levels.
Conclusion. Decreased hip ROM may be considered an aetiological factor in the occurrence of adductor strain in male professional soccer players.
Keywords: groin; hip joint; range of motion, articular; soccer; sprains and strains
Introduction
Soccer is the world’s most popular sport; its activity involves running, kicking, stepping, jumping, and cutting, which may lead to a number of lower limb injuries.1,2 Groin injuries account for 10 to 18% of all soccer injuries.3–5 The causes of groin pain can be multiple and 27% of athletes have more than one cause of groin pain.6 Strain of any of the 3 adductors (adductor longus, adductor brevis, adductor magnus) has been suggested as the main cause of groin pain in soccer players5 and ice skaters.7 Risk factors for adductor strain include adductor tightness,8,9 previous adductor injury,7 and hip adductor-toabductor strength imbalance.7 Despite identification of risk factors and implementation of preventative programmes, adductor strains continue to occur in sporting activities.10,11 Decreased range of movement (ROM) of the hip has been suggested as a risk factor for sports-related chronic groin pain in athletes.12
Decreased internal rotation and ROM of the hip are associated with chronic groin pain. Patients who have recovered from groin pain have a greater hip ROM than those who are still having pain.
This study aimed to determine whether adductor strain in soccer players is associated with a decreased ROM, and whether injured players regain their hip ROM after resolution of the adductor strain.
Methods
Ethics approval for study on human subjects was obtained from the South Eastern Health Human Research Ethics Committee, Southern Section prior to the commencement of the study. All subjects gave written informed consent before inclusion.
Before the 2003–2004 Australian National Soccer League season, 120 potential subjects were recruited from 6 professional soccer teams to fill out a questionnaire to assess their eligibility for the study. All had their preseason hip ROM (internal plus external rotation) measured by a single examiner. Subjects with a history of groin or adductor strain were included. They were asymptomatic at the start of the soccer season and did not have pain for over one year.
An injury was defined as any event that kept a player out of practice or games for at least one week. An adductor strain was defined as pain on palpation of the adductor tendons or their insertion on the pubic bone or both, and groin pain during adduction against resistance.7,10 Adductor strain grading was per protocol described by Speer et al.13
Injured subjects were re-examined within 72 hours to confirm eligibility and make further measurements. Ultrasound and/or bone scintigraphy were used to assess pathology and determine muscle strain category. Changes in hip ROM during injury, immediately after recovery, and at the end of the season were recorded. Recovery was defined as return to full training or playing of a full match. For all players with possible adductor strain, a thorough history was obtained and a clinical examination performed to differentiate adductor strain from other causes of groin pain.7,10
The athlete was placed in a supine position and the relevant hip and knee were flexed to 90º. Passive internal and external rotation of the hip was performed bilaterally to the end range using a standard goniometer, with the mean of 3 measurements recorded. To assess intra-observer reliability, 20 subjects were re-tested one week after initial measurements prior to the start of the season by the same examiner.
Intraclass correlation coefficients (ICCs) were recorded with 95% confidence intervals to measure the test-retest reliability of hip measurements. Hip ROMs of the injured and uninjured sides of the injured group were compared using paired sample tests. Comparison of mean hip ROMs between injured and uninjured groups was made using independent samples t-tests. A p value of <0.05 was considered significant.
Results
Of the 120 potential subjects, 19 were excluded because they were traded overseas (n=4), cut from the team squad (n=10), or resigned from playing due to other medical issues (n=5). Eight of the 101 players (9 injuries) met the inclusion criteria.
The ICC was 0.88 in internal rotation and 0.96 in external rotation. 22 players had groin injury; 8 of them had 9 injuries that kept them out of practice for at least one week; 10 had groin injuries that resolved within 3 to 5 days; one had 2 episodes of groin pain on different sides; 2 had inguinal hernias and another 2 had osteitis pubis.
The mean preseason hip ROM of the 8 injured players was significantly lower than that of the uninjured group (44.7º vs 53.7º; injured dominant leg, p=0.03; injured non-dominant leg, p=0.04). Among players sustaining adductor strain, the difference of preseason ROM between the injured and uninjured side was significant, with the injured side 3º less than the uninjured side (p=0.06). In uninjured players (n=93), the difference between dominant and nondominant side was not significant (53.3º vs 56º, p=0.65).
Seven adductor strains were of grade I, and 2 were of grade II; no grade III strains were reported. These represented 2.78 adductor injuries per 1000 playing hours. The total number of matches missed was 20.
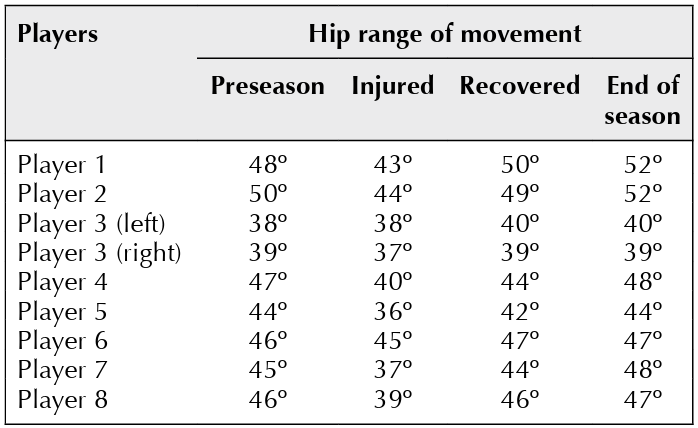
Respective hip ROM results on the side sustaining the injury are shown in the Table. Seven hips had a decrease in ROM soon after the injury; 6 had an increase in ROM at the end of the season.
Three (38%) of the 8 players in the injured group had a history of groin pain that forced them to miss game time in previous seasons, compared to 28 (31%) of 91 in the uninjured group.
Table Hip range of movement in 8 players with adductor muscle strain
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Discussion
Groin pain affects 10 to 18 per 100 soccer players per year.2,3,14 Groin injuries in soccer matches account for 5 to 13% of all musculoskeletal injuries.1,5 It is difficult to classify groin pain and many studies refer to a heterogeneous group of conditions that manifest as groin pain, including osteitis pubis, hernias, hip pathology, and stress fractures of the pelvis. It is therefore difficult to compare previous studies. The present study concentrated on a single component of groin pain—adductor strain, as it is a major cause of symptoms in this sporting population.6
Previous studies have shown an association between strength and/or flexibility and musculoskeletal strains in various athletic populations.1,4,15 For adductor strains, identified risk factors were: inflexibility of the adductor tendon,1 weakness of the adductor tendon,7 and previous adductor strain and injury.7,16
In soccer players, a correlation has been described between tightness of the adductors and the presence of adductor strain.8 Tyler et al.7 showed that preseason weakness in adductor strength and a weak adductor-to-abductor ratio of <80% was prognostic of adductor strain. This study also assessed flexibility of the adductor but did not demonstrate a correlation between inflexibility and adductor strains. Witvrouw et al.17 also failed to show adductor inflexibility as a significant factor leading to groin pain.
Players with previous adductor strains were included. Both the injured and uninjured groups had experienced a similar prevalence of previous groin injury (38% vs 31%), which justified the inclusion of previously injured players in the study. Seward et al.16 reported a 32% recurrence rate for groin strains in Australian Rules Football over 12 months. Tyler et al.7 recorded a 44% recurrence rate of groin injuries in ice hockey players over 24 months.
The link between hip ROM and adductor strain has not been described and is not entirely clear. Fricker et al.18 proposed a mechanism whereby the hip joint undergoes inflammation and scarring as part of an overuse syndrome akin to the frozen shoulder (which follows rotator cuff injury). Either from vascular deprivation of pelvic structures or from sites of inflammation in the hip, the resulting stiffness is a manifestation of reflex muscle spasm of hip rotators, flexors, and adductors. This may explain why after the onset of adductor strain, there is a further decrease in hip rotation, pain on hip movement, and associated weakness of adduction. When the acute phase of injury has subsided, the hip rotation returns to its pre-injury ROM. Mechanisms for this return to pre-injury ROM, though not entirely clear, include aggressive rehabilitation regimens, rest or the removal of pain inhibition cycles.
The adductors have been shown to cause internal rotation of the hip in the extended position.19 This contraction of the adductor group against a stiffened hip capsule may well be another cause of adductor strain. Williams20 proposed that sporting activities such as soccer require free internal rotation of the hip joint in both flexion and extension. Whenever such movement is restricted, stress is applied across the hip joint to the hemipelvis on the opposite side.
Conclusion
Reduction of hip ROM may be considered an aetiological factor in the occurrence of adductor strain in professional soccer players. Thus, ROM testing may be useful to consider in the standard battery of preseason assessments used by most soccer clubs. Future prospective study is needed to determine whether appropriate interventions directed at players with limited hip ROM leads to a decrease in adductor strain.
References
- Ekstrand J, Gillquist J. Soccer injuries and their mechanisms: a prospective study. Med Sci Sport Exerc 1983;15:267–70.
- Nielsen AB, Yde J. Epidemiology and traumatology of injuries in soccer. Am J Sports Med 1989;17:803–7.
- Holmich P. Adductor related groin pain in athletes. Sports Med Arthrosc Rev 1997;5:285–91.
- Dvorak J, Junge A, Chomiak J, Graf-Baumann T, Peterson L, Rosch D, et al. Risk factor analysis for injuries in football players. Possibilities for a prevention program. Am J Sports Med 2000;28(5 Suppl):S69–74.
- Renstrom P, Peterson L. Groin injuries in athletes. Br J Sports Med 1980;14:30–6.
- Lovell G. The diagnosis of chronic groin pain in athletes: a review of 189 cases. Aust J Sci Med Sport 1995;27:76–9.
- Tyler TF, Nicholas SJ, Campbell RJ, McHugh MP. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med 2001;29:124–8.
- Ekstrand J, Gillquist J. The avoidability of soccer injuries. Int J Sports Med 1983;4:124–8.
- Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med 2004;32(1 Suppl):S5–16.
- Holmich P, Uhrskou P, Ulnits L, Kanstrup IL, Nielsen MB, Bjerg AM. Effectiveness of active physical training as treatment for long standing adductor-related groin pain in athletes: randomised trial. Lancet 1999;353:439–43.
- Tyler TF, Nicholas SJ, Campbell RJ, Donellan S, McHugh MP. The effectiveness of a preseason exercise program to prevent adductor muscle strains in professional ice hockey players. Am J Sports Med 2002;30:680–3.
- Verrall GM, Hamilton IA, Slavotinek JP, Oakeshott RD, Spriggins AJ, Barnes PG, et al. Hip joint range of motion reduction in sports-related chronic groin injury diagnosed as pubic bone stress injury. J Sci Med Sport 2005;8:77–84.
- Speer KP, Lohnes J, Garrett WE Jr. Radiographic imaging of muscle strain injury. Am J Sports Med 1993;21:89–96.
- Holmich P, Holmich LR, Bjerg AM. Clinical examination of athletes with groin pain: an intraobserver and interobserver reliability study. Br J Sports Med 2004;38:446–51.
- Orchard J, Marsden J, Lord S, Garlick D. Preseason hamstring muscle weakness associated with hamstring muscle injury in Australian footballers. Am J Sports Med 1997;25:81–5.
- Seward H, Orchard J, Hazard H, Collinson D. Football injuries in Australia at the elite level. Med J Aust 1993;159:298301.
- Witvrouw E, Danneels L, Asselman P, D’Have T, Cambier D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players. A prospective study. Am J Sports Med 2003;31:41–6.
- Fricker PA, Taunton JE, Ammann W. Osteitis pubis in athletes. Infection, inflammation or injury? Sports Med 1991;12:26679.
- Kendall FP, McCreary EK. Muscles: testing and function. 4th ed. Baltimore: Williams & Wilkins; 1993.
- Williams JG. Limitation of hip joint movement as a factor in traumatic osteitis pubis. Br J Sports Med 1978;12:129–33.